Crestal Sinus Floor Elevation


Double crestal sinus floor elevation
Clinical challenge
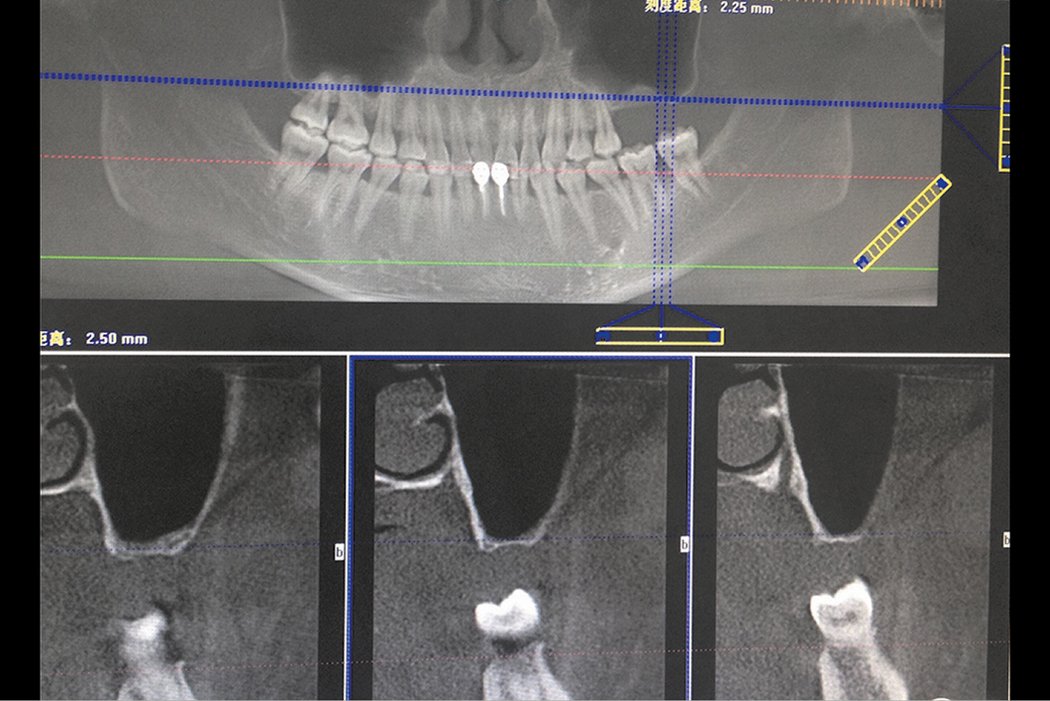
Alveolar bone resorption in posteriormaxilla and maxillary sinus pneumatization always challenges the implant placement. Maxillary sinus floor elevation and onlay bone grafting are the regular methods for solving these problems. Two main approaches for the maxillary sinus floor elevation procedure are now widely used in dental clinics. Lateral antrostomy is mostly used in severe alveolar bone resorption but one of the drawbacks of the lateral antrostomy is that it requires the raising of a large flap for surgical access. The crestal approach is considered to be a more conservative method. This case report demonstrates a minimally invasive technique for the management of vertical ridge defects (less than 1mm) in the posterior maxilla. The double-crestal-approach provides clinicians a simple, convenient and minimally invasive approach compared to the regular lateral antrostomy.



Clinical outcome at a glance
Objectives
- Dual sinus floor elevation with dual-crestal approach using Geistlich Bio-Oss® and Geistlich Bio-Gide®
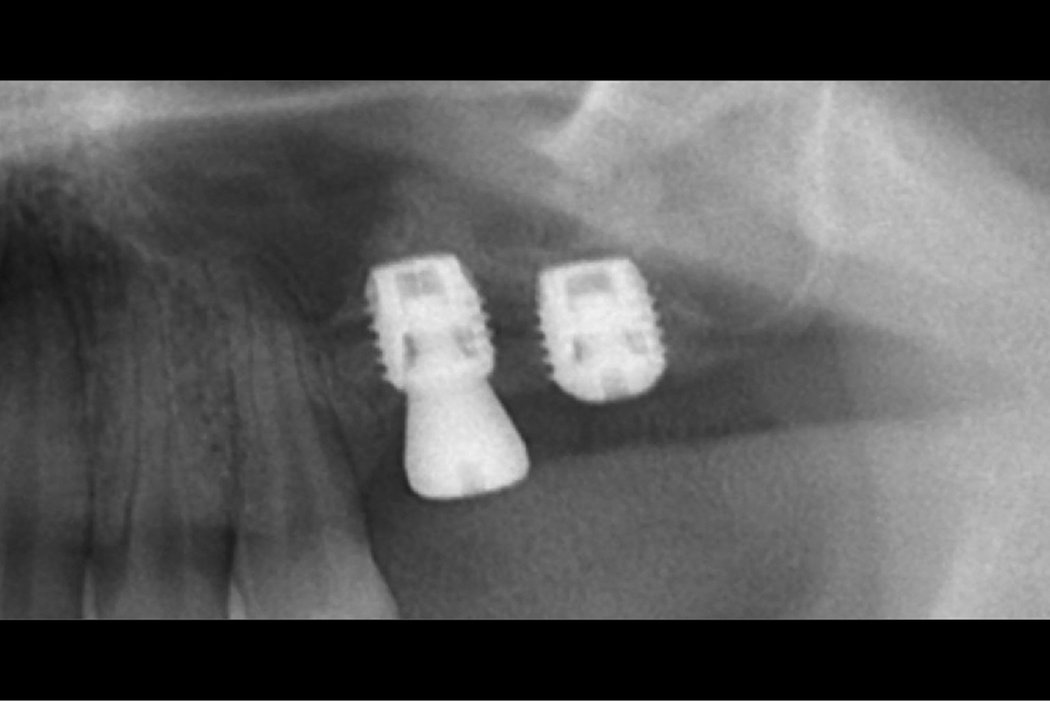
- Short implant placement due to severe bone resorption
Conclusions
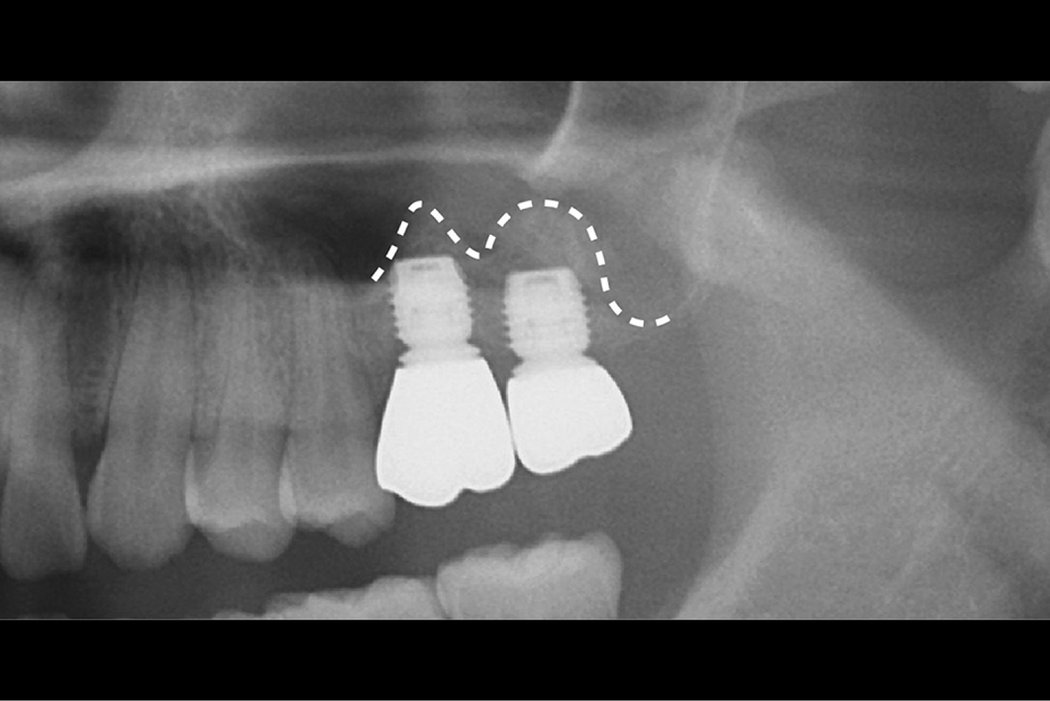
- Dual-crestal sinus floor elevation using Geistlich Bio-Oss® and Geistlich Bio-Gide® in combination with short implant placement overcome severe bone resorption
- Fewer postoperative complications using Geistlich biomaterials in combination with dual-crestal sinus floor elevation
Aim / Approach
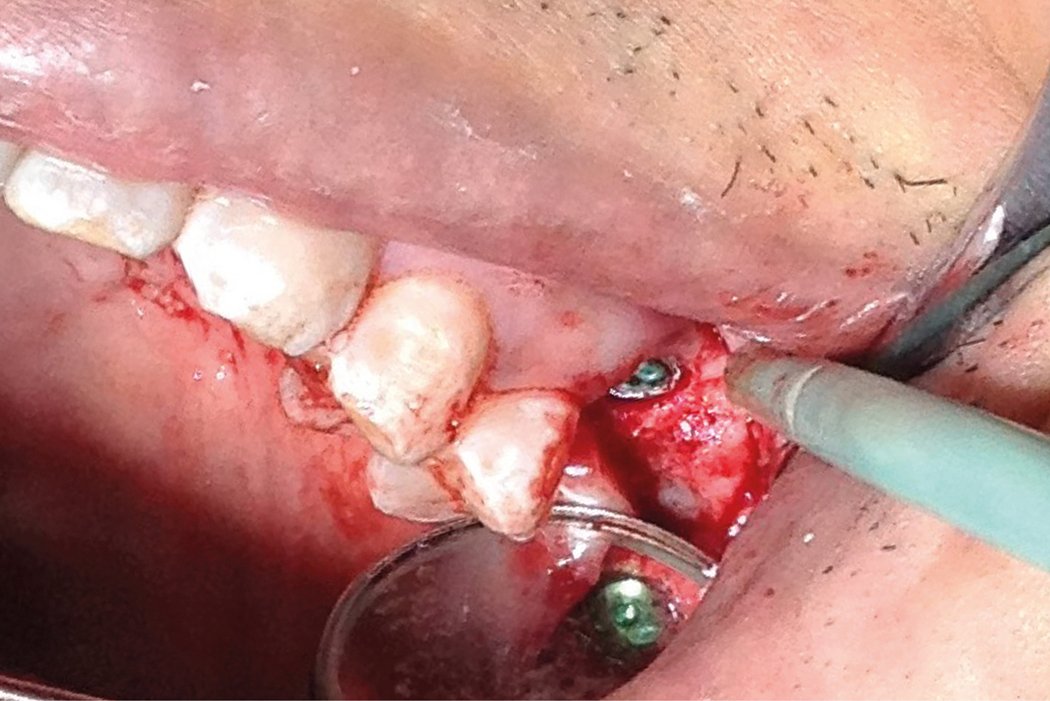
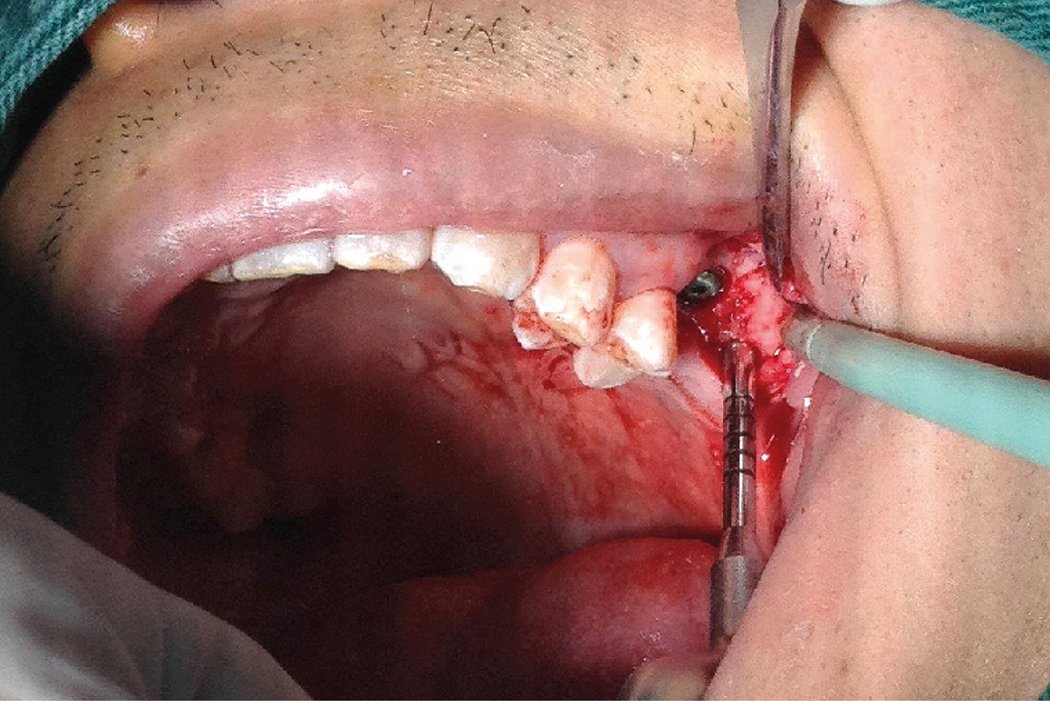
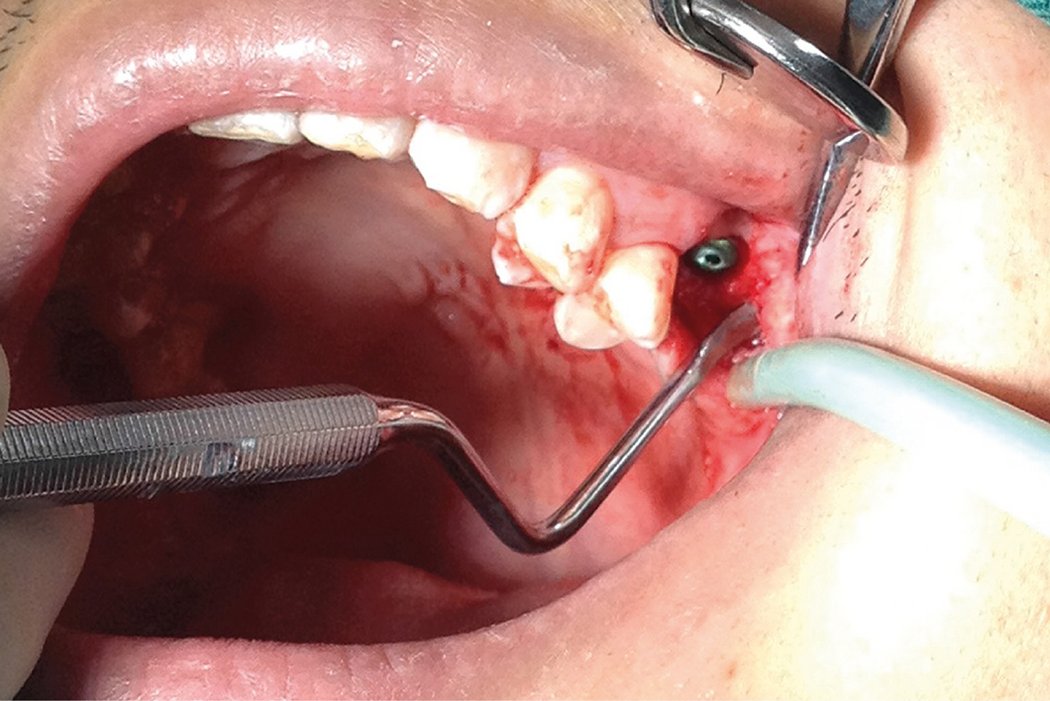
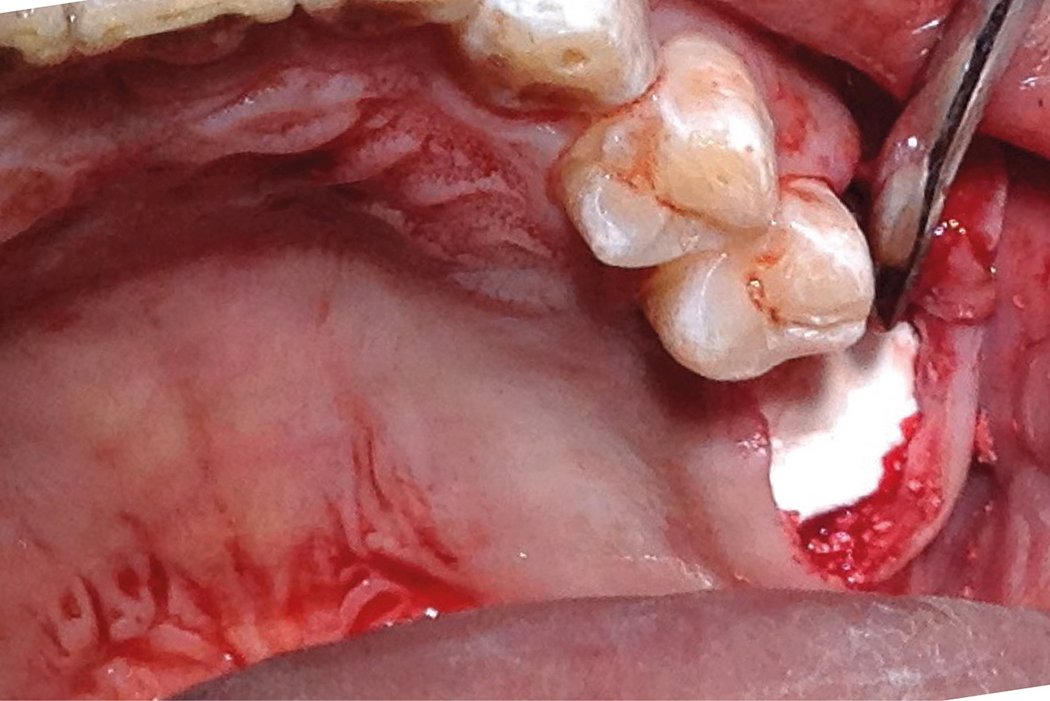
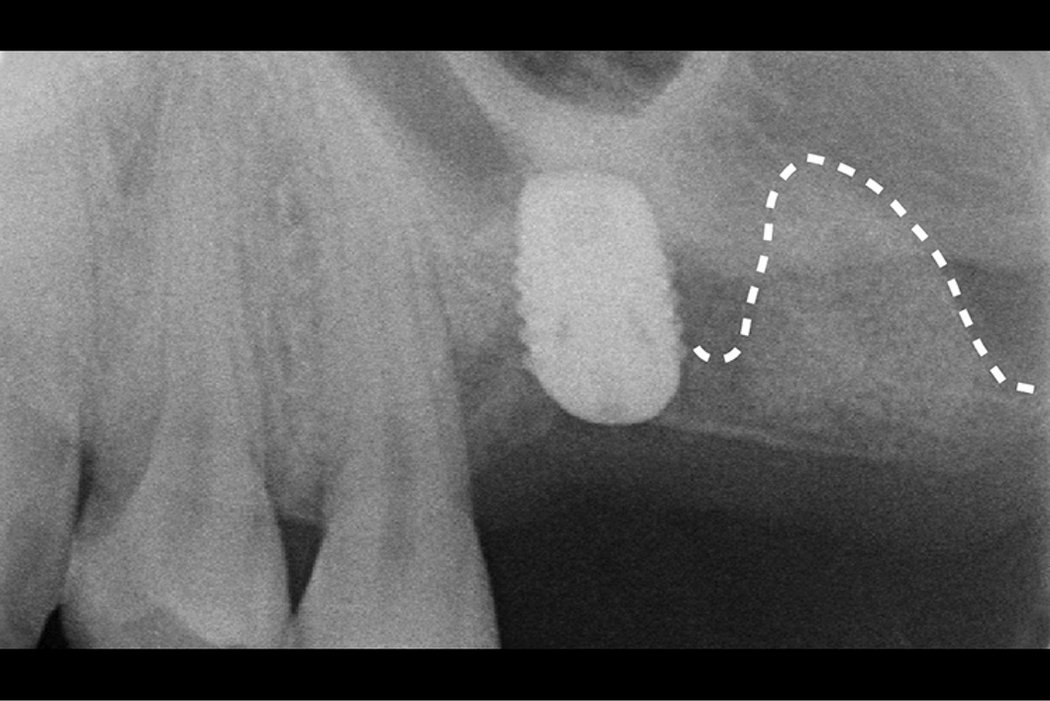
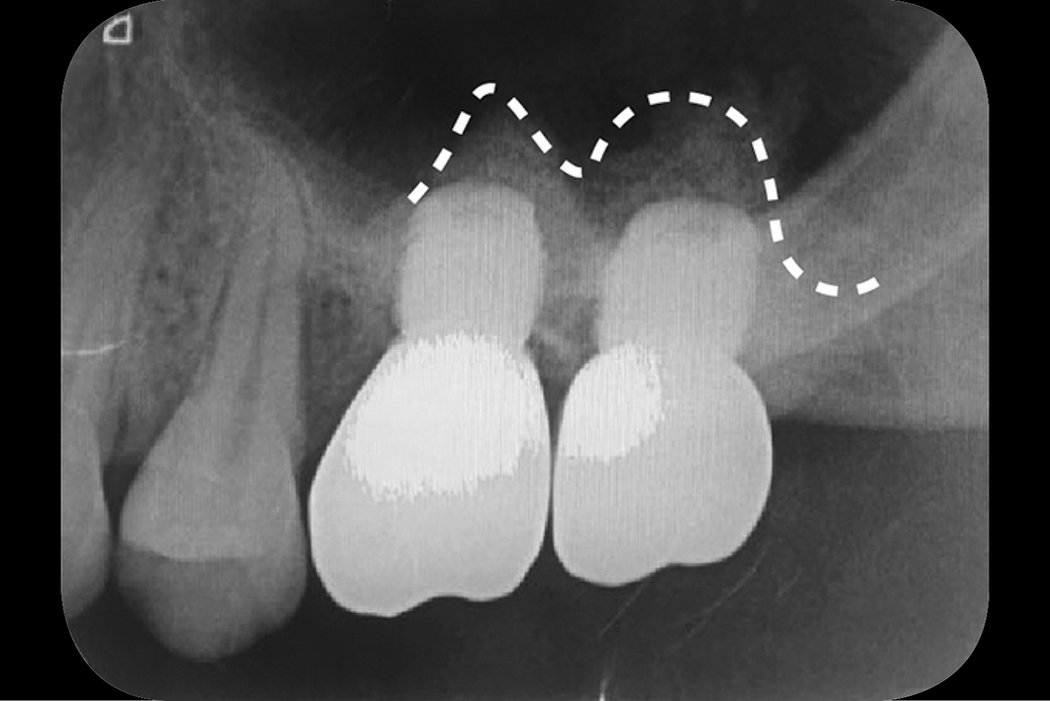
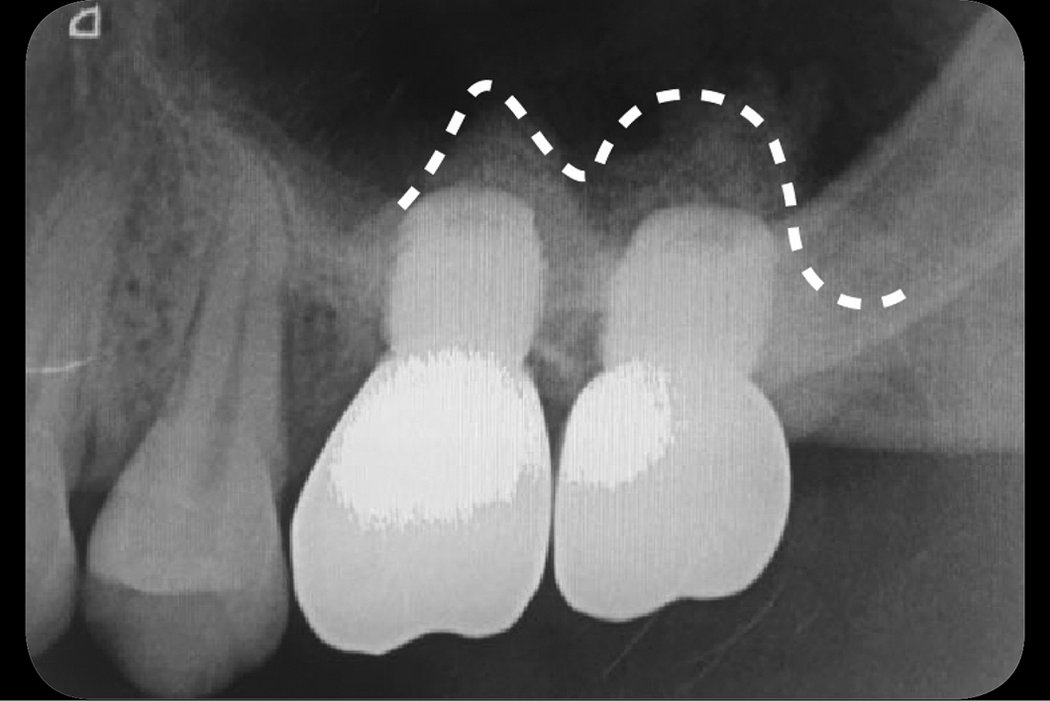
Treatment was carried out under local anaesthesia with local buccal and palatal infiltrations. The proposed implant site was marked with a trephine drill. The depth was controlled within the alveolar bone to protect the sinus membrane from perforation. Then the round bone block was gently tapped and pushed into the maxillary sinus using the sinus lift osteotome. By using the trephine drill, the cut bone block can be used. While the bone block was gently pushed into sinus, the sinus membrane was elevated at the same time. The boneblock provides the osteoblast while the connected sinus membrane provides the blood supply. The osteoblast and blood supply are the key factors forbone ossification. The Schneiderian membrane near to the bone block was slightly dissected using an antralcurette. Then the bone block was elevated again for about 4mm. A spaceis created by the intruded bone block. This space is then grafted with Geistlich Bio-Oss®. Geistlich Bio-Gide® was adapted too verlay the osteotomy site. The second sinus floor elevation was performed six months later with the same procedure.
Conclusion
The dual-crestal approach combined with the placement of a short implant is an efficient method for overcoming the severe posterior maxilla bone resorption. Elevating the sinus floor by a crestal approach twice reduces the use of bone grafting material, saves surgical time and cost, and leads to fewer postoperative complications.